The post Results from the NASH-FX Study Underscore the Importance of Completing the NASH-CX Clinical Trial for Patients with NASH Cirrhosis appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The NASH-FX study was designed as a pilot study at a single site, involving only four months of treatment with GR-MD-02. This pilot study evolved from the results of a Phase 1 study in NASH patients with advanced fibrosis that had suggested FibroScan® measurements improved in three patients with just four doses of the study drug. The full report of this Phase 1 study will be published in the next few weeks in the peer-reviewed scientific journal, Alimentary Pharmacology and Therapeutics.
While most experts feel that liver fibrosis trials should have treatment phases for at least a year in duration, the results from the earlier Phase 1 NASH study provided a rationale for studying a larger group of patients with shorter therapy and exploring non-invasive technologies for assessing liver disease and fibrosis with a goal of using these technologies in later trials.
I want to give you a few details on the design of the NASH-FX study. The primary endpoint of NASH-FX was the LiverMultiScan (LMS), an approved magnetic resonance imaging test developed by Perspectum Diagnostics to assist in the diagnosis of liver disease. In NASH, the LMS is reported to measure the amount of fibrosis and inflammation. The LMS has low variability between scans in the same individual, and we used this low variability to calculate the number of patients we would need for the study to show a statistically significance difference between treatment groups with a power of 80%. In other words, the study was designed to have an 80% chance of showing a statistically significant difference in a 30 patient study, with 15 placebo and 15 GR-MD-02 patients. The power of the actual study, calculated after completion, was almost exactly an 80% chance to show an approximately 10% difference in LMS between placebo and treated groups. Therefore, the study design was adequate for the primary endpoint.
In contrast to LMS, the study was not powered for the secondary endpoints of liver stiffness, FibroScan and magnetic resonance elastography (MRE). The study would have required between 3 to 5 times as many patients to have an adequate power to show a difference with these tests. This is because the variability of these tests for repeated measurements is considerably greater than LMS.
However, we did not know before we conducted the study, nor did anyone else know, whether LMS correlated with the liver stiffness measurements of FibroScan and MRE. The NASH-FX study showed that there was poor correlation. Therefore, one cannot conclude that because there was no difference in LMS, that there would not be a difference in stiffness measurements, which have been shown in liver biopsy studies to correlate with fibrosis.
Although there was no apparent improvement in the three non-invasive tests for assessment of liver fibrosis in the four-month NASH-FX study, Dr. Stephen Harrison, a leading investigator in NASH and liver disease and the principal investigator of the NASH-FX study has pointed out that the inhibition of galectin-3 with GR-MD-02 remains promising for the treatment of NASH fibrosis. Dr. Harrison was especially encouraged that GR-MD-02 has demonstrated an improved clinical effect in moderate-to-severe psoriasis, suggesting the compound has activity in a human disease that can occur in association with NASH.
It remains critical that we complete the longer therapy NASH-CX clinical trial that has a much larger group of patients with NASH cirrhosis.
The NASH-CX trial is a one-year of treatment, multi-center trial in patients with NASH cirrhosis that is being conducted at 36 outstanding liver centers in the United States. The endpoints of the NASH-CX trial include invasive tests that are well-validated measures of liver disease severity. The primary endpoint is the change from baseline in the hepatic venous pressure gradient (HVPG), which measures the blood pressure in the liver and is well correlated with the clinical outcomes of patients.
Liver biopsy is an important secondary endpoint in the NASH-CX trial, which evaluates the stage of liver fibrosis and the amount of collagen, the primary component of fibrotic tissue. Finally, there are also non-invasive tests as secondary endpoints, including FibroScan and the 13C-methacetin breath test, which measures the metabolic function of the liver. These are important to correlate with the invasive tests because they may be useful in future trials and in management of patients.
I am pleased to report additional information on the status of this most important clinical trial as of October 10, 2016:
- The NASH-CX trial completed enrollment one month early with 162 total patients, exceeding the target of 156. This keeps us well on track for reporting of top-line results in December of 2017.
- The 162 patients were enrolled at 36 sites in the United States following the screening of 290 patients to obtain a population with well-compensated NASH cirrhosis (Child-Pugh-Turcotte Class A) with elevated portal pressure (HVPG ≥ 6 mmHg).
- In determining the number of patients to meet statistical requirements, we planned for the possibility that as many as 25% of the patients may drop out of the study during the treatment phase. However, we are pleased that only five patients of the 162 enrolled have dropped out of the study thus far. This low attrition rate highlights the importance, urgency, and need for patients suffering from NASH-cirrhosis to find an effective medical treatment.
- The low drop out trend also suggests that we will have a robust number of patients completing treatment for evaluation at the end of the trial. The trial was designed to have an 80% chance of demonstrating a 2 mmHg reduction in HVPG (i.e. 80% power) with 117 patients evaluated. Any number of patients above 117 will simply enhance the power of the study.
- At this point, 4 patients have completed the entire protocol and 70 patients have already completed six months of dosing.
- A total of 2,000 drug infusions (including placebo) have been given in this trial, representing 48% of the total number of infusions in the entire study. So we are quite pleased that this study is well along in its development.
The safety and tolerance of GR-MD-02 in all of the trials is most encouraging and supports our commitment to pursue the lead indication of NASH cirrhosis. In the NASH-FX study, GR-MD-02 was found to be safe and well-tolerated among the patient population with no serious adverse events related to the study medication. Over all of the clinical trials, including the patients in the NASH-CX trial, more than 1600 doses of GR-MD-02 have been administered without serious adverse effects related to the drug. This highlights the superior safety profile of the therapy in a patient population with advanced-stage disease, which is buttressed by the biological activity demonstrated in patients with moderate to severe plaque psoriasis.
Dr. Harrison, one of the two co-lead investigators in the NASH-CX trial, stated his belief that the inhibition of galectin-3 with GR-MD-02 remains a promising treatment for NASH fibrosis and that it is important to complete the NASH-CX trial.
Dr. Naga Chalasani, the other co-lead principal investigator of the NASH-CX trial, provided his assessment, stating:
“The results from the NASH-FX trial do not diminish the significance of the NASH-CX trial. Along with the safety and tolerability profile observed in the NASH-FX trial, the different patient population, much larger enrollment, rigorous study design and longer duration of therapy offer compelling rationale to complete the NASH-CX trial.”
As a company, Galectin Therapeutics’ attention has always been focused on completing the NASH-CX clinical trial and reporting results in a timely fashion.
With an outstanding safety profile, inhibition of galectin-3 with GR-MD-02 remains a potential treatment of NASH cirrhosis. Additionally, the longer therapy for one year, and endpoints that may serve as a surrogate for outcomes for registration trials in this patient population, provides us encouragement about our continuation of NASH-CX clinical trial.
These “CEO Perspectives” are a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, including whether GR-MD-02 may be effective in the treatment of NASH. These statements relate to future events and use words such as “may,” “might,” “could,” “expect” and others. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2015, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Make a Comment or Ask a Question
[contact-form-7]The post Results from the NASH-FX Study Underscore the Importance of Completing the NASH-CX Clinical Trial for Patients with NASH Cirrhosis appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Love Your Liver: A Prescription for Liver Health appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>I am often asked how one can maintain a healthy liver and avoid the complications that can happen with chronic fatty liver disease. It has also recently been shown that fatty liver disease is an independent risk factor for cardiovascular disease, providing everyone with another important reason to maintain a healthy liver.
Liver health should be as important to everyone as heart health. However, how do you go about ensuring that your liver is healthy? I have listed below my suggested steps to maintain a healthy liver.
Maintain a healthy weight
There is a clear connection between body weight and the risk of NASH, including an increase in organ fat in apparently lean people (see here). If you are overweight, losing as little as 10% of your body weight can result in a much healthier liver (see here).
Follow a healthy diet
It is not my intention to provide specific dietary advice, but your liver diet should be preferably high in lean protein, low in carbohydrate like starch, low in added sugar, and limited high fructose corn syrup.
Exercise
Activity appears to improve fatty liver disease and help keep your liver healthy even if you don’t lose weight. Studies show resistance exercise is as beneficial as aerobic exercise.
Avoid excessive alcohol
Know the exact alcohol content of what you are drinking and what constitutes a “drink.” Men should drink a maximum of two drinks a day and women should limit themselves to one drink a day.
Avoid certain nutritional supplements
Certain nutritional supplements and herbal remedies can damage the liver. Talk to your doctor or read on-line about all supplements you are considering. For example, even too much iron or vitamin A can be harmful to your liver.
No illicit drug use
This may seem obvious, but you must avoid the use of drugs that expose you to blood from others, which put you at risk for hepatitis.
Discuss liver health with your doctor
Ask your primary care doctor, “How’s my liver?” You will often have gotten routine blood tests that include liver enzymes that may provide an indication of liver problems. Also, always ask whether there are potential liver effects from drugs, over-the-counter medicines, nutritional supplements and vitamins you may be taking.
These all seem like simple steps, but if everyone were following them we would not have the epidemic of fatty liver disease and other liver diseases we have today. Consider incorporating these steps in your lifestyle today.
These “CEO Perspectives” are a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “might,” “could,” “expect” and others. For a discussion of factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2015, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Make a Comment or Ask a Question
[contact-form-7]The post Love Your Liver: A Prescription for Liver Health appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Can Thin People Get Fatty Liver Disease? Lean NASH appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>I suppose it’s natural to assume that only overweight people get fatty liver disease (and NASH), but one thing I have learned over my career in medicine is to always challenge such “common sense” assumptions with empirical research. It turns out that, while people who are overweight or obese are indeed at greater risk, thin people can also develop fatty liver disease, NASH and cirrhosis. This has come to be known as “lean NASH.”
The commonly accepted definition of obesity is a body mass index (BMI) of 30 or more. However, overall BMI is less important in determining risk for fatty liver disease than where the fat is located in the body. Visceral fat, when the fat is nestled in and around the organs of the belly, is more strongly linked to fatty liver disease and other metabolic disorders than fat in arms, legs, and other parts of the body. A person can easily have a BMI well below 30 and still have considerable visceral fat. Someone who is “metabolically obese, normal weight” will have many of the hallmarks of obesity, such as insulin resistance (requirement of higher insulin levels to control blood sugar), metabolic syndrome (high blood sugar, elevated fats and cholesterol in blood, high blood pressure, and excess body fat around the waist) and NASH.
A study published in 2012 showed that overall prevalence of fatty liver disease among obese individuals was 28 percent, while fatty liver disease was identifiable in 7 percent of the lean individuals tested. (Zobair M. Younossi, 2012) Yes, obese people had a greater incidence of fatty liver disease, but lean people still showed a surprisingly high prevalence of the disease.
The other surprising finding from this study was that lean NASH patients here in the U.S. tend to be Hispanic. It’s unclear whether it is culture, diet, genetics, or some completely different mechanism at work that makes those of Hispanic ancestry more likely to develop lean NASH. But, given the growth of the Hispanic population here in the U.S., lean NASH is likely to emerge in the coming decades as an important cause of chronic liver disease.
Ethnicity does seem to be one of the major determinants of lean NASH, which was first described by physicians in Asia. While metabolic syndrome has long been a problem in developed countries, it is an increasing problem in developing countries as well, even though the rate of obesity remains comparatively low. The prevalence of fatty liver disease among normal-weight individuals was recently reported at 12% in Greece, 20% in India and 15% in China.
One analysis from 2013 suggests that lean NASH, as seen in Asia, is a distinct phenotype of NASH (Kausik Das, 2013). Asians, this study notes, show a propensity to develop metabolic syndrome at a lower BMI. One possible reason is that early malnutrition, either in utero or in early childhood, primes the body to store visceral fat more aggressively. The relative abundance of food in Asia today over the scarcities common only a few decades ago means that adults in China, India and other Asian countries are increasingly at risk of developing lean NASH.
I’ve called fatty liver disease a “hidden epidemic,” and lean NASH is even more so. It is easy to identify someone with a high body weight as being at risk for fatty liver disease, but less so for someone with lean NASH. We need a much better understanding of what causes lean NASH and how its presentation and biomarkers are distinct from the fatty liver disease and NASH seen in overweight patients.
Works Cited
- Kausik Das, A. C. (2013). Lean NASH: distinctiveness and clinical implication. Hepatol Int , 7(Supplement 2), S806 – S813.
- Zobair M. Younossi, M. M. (2012, November). Nonalcoholic Fatty Liver Disease in Lean Individuals in the United States. Medicine, 91(6), 319-227.
These “CEO Perspectives” are a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “might,” “could,” “expect” and others. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2015, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Make a Comment or Ask a Question
[contact-form-7]The post Can Thin People Get Fatty Liver Disease? Lean NASH appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post The Dilemma of Treating NASH appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>You may have seen Newsweek’s recent article on the growing impact of NASH, NASH Is the 21st Century’s Looming Health Threat. It’s a great article that vividly demonstrates the heartbreak of a NASH diagnosis and the shame and uncertainty faced by many patients.
“I’m in this situation and not for lack of good diet and exercise,” says Sandra, whose father died of liver disease 30 years ago. “You can blame me if you like, but I’m doing what I’m supposed to do.”
“Unlike those who suffer from other serious illnesses, NASH patients have no colored wristband denoting awareness, no annual fundraising race, no built-in support network.”
This article has gotten me thinking about ethical issues surrounding treating NASH and fatty liver disease.
There was a hint in the Newsweek article of the debate over whether medical intervention in NASH is at some level a questionable endeavor, as it may make better sense for society to address the epidemic of obesity directly rather than try and deal with NASH. However, that argument doesn’t hold up under scrutiny, as nearly 50% of the U.S. population is overweight or obese by the standard definitions. If you refused to treat medical problems that arise due to, or are exacerbated by obesity that would mean you wouldn’t treat heart disease, diabetes, or osteoarthritis. Even cancer is closely related to obesity and diet. Additionally, as I will elaborate on in a future CEO Perspective, lean people can also suffer from NASH so it is a lot more complicated than just a fat liver.
I wrote recently about how fatty liver disease helped motivate me to lose weight. I believe that awareness and lifestyle changes, including weight loss and exercise, will always be the best ways for the medical community and healthcare in general to address the looming health crisis of fatty liver disease. A recent study showed that a 10% reduction of body mass resolved NASH in 90% of the patients in the study.
However, I also remain convinced that there will always be a need for direct drug intervention for NASH. Not everyone will respond to a regime of weight loss and increased exercise. NASH is a progressive disease, and the question becomes: At what stage do we resort to direct medical intervention rather than focusing on lifestyle changes?
There was a study published last year in Hepatology [1] that took patients with a biopsy-proven diagnosis of NASH and followed them for up to 33 years, with an average of 26 years. This study was done in Sweden, so it was easier to track patients for that length of time than it might be here in the U.S. The study showed that if a patient started with stage 1 or 2 disease (mild fibrosis), they had no increased risk of mortality in comparison to a reference group. Let me repeat: Fatty liver disease itself didn’t affect patient mortality at all when followed for up to 33 years! However, if a patient had advanced fibrosis — stage 3 and 4 disease — they had a 3.3 times increase in mortality over the reference population.
To me, this study suggests that it would questionable to undertake a broad pharmaceutical approach to managing early-stage NASH. While a certain percentage of people will progress to advanced-stage NASH, we currently have no way of predicting which patient is at risk for this. Is it worth treating all 30 million people in the US with NASH, exposing them to the expense of the medication and its inevitable side effects when the treatment is not likely to have any impact on their long-term morbidity or mortality?
In contrast, we know that those who have NASH with advanced liver fibrosis do have an increase in morbidity and mortality related to NASH, so the more desirable approach might be to have a noninvasive test that can distinguish early-stage NASH from late-stage NASH and a follow-up treatment with a drug proven to be efficacious for late-stage NASH.
Galectin Therapeutics is distinctive among the companies developing therapies for treatment of NASH because we are focused exclusively on treatment of late-stage NASH with advanced fibrosis and cirrhosis. We have done this for the medical reasoning outlined here and the fact that the preclinical efficacy of our drug GR-MD-02 has a differentiated profile from other drugs in development in that it both prevents and reverses liver fibrosis. I think the science, the medical decision making, and ultimately the market will bear out that this is the point of greatest need.
- Journal of Hepatology, Volume 62, Supplement 2, April 2015, Pages S362–S363
Make a Comment or Ask a Question
[contact-form-7]The post The Dilemma of Treating NASH appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Developing Tests to Assess Liver Function in NASH and Cirrhosis appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>I wrote recently about the need for non-invasive tests to replace liver biopsies in the evaluation of liver fibrosis due to various diseases, including NASH, and I also spent time exploring some of the non-invasive serum and imaging tests that are in development. I started this whole discussion by stating that it is difficult to assess liver function and the effect of fibrosis on liver function. As a result, we must rely on direct physical assessments like biopsy and imaging tests and indirect evaluations like serum tests, which attempt to provide insight into what is going on in the liver. Yet there are a number of potential approaches to testing actual liver function being developed, and we are evaluating one of these in the course of our own clinical trials.
For example, one of the functions of the liver is to extract bile acids out of serum and excrete them into the bile that then enters the intestine. A company called HepQuant, headed by Dr. Greg Everson, whom I’ve known for many years, has developed a test for this. A small intravenous dose of a non-radioactive labeled bile acid and an oral dose are administered to the patient and the test then measures how well the liver takes up this bile acid.
HepQuant has generated data that demonstrate a linear correlation between its test’s results and various measures of liver disease, such as degree of fibrosis. Unfortunately, the test wasn’t ready for use when we started our clinical trials, but the HepQuant test could be a very important endpoint in the future. [1]
Another function of the liver is to metabolize drugs. A 13C-methacetin breath test developed by Exalenz Bioscience measures the metabolism of a drug, and we are making use of this test in our NASH CX trial. Developers have been pursuing this approach for many years, but it has only recently come into clinical use. [2]
The concept behind the 13C-methacetin breath test is that the liver metabolizes a drug called methacetin into acetaminophen. We’re probably all familiar with acetaminophen, which is sold over-the-counter as Tylenol®. Methacetin has been available for a long time as an oral drug for pain relief, but it’s not in high demand now because people tend to use acetaminophen as a first choice. In metabolizing methacetin, the liver uses an enzyme called cytochrome P450 1A1 to remove a methyl group off methacetin, which results in acetaminophen.
The amount of cytochrome P450 in the liver is related to liver disease, and the amount decreases as the severity of the disease increases. The liver has a tremendous capacity for metabolizing drugs, but with a sufficiently sensitive test, even small changes in the metabolic capacity can be identified before they become a big problem.
In the Exalenz 13C-methacetin breath test, the methyl group on the methacetin has been tagged with a carbon-13 (13C) atom, rather than the normal carbon-12 atom. You may recall from chemistry class that carbon-14 is a radioactive form of carbon, but carbon-13 is not. The 13C-laced methacetin is given to the patient orally. The liver metabolizes the methacetin by knocking off the methyl group, which is turned into 13C-laced CO2 and passes through the blood stream to be exhaled. The patient wears a nasal cannula and breathes normally, and a machine measures the amount of carbon-13 that is excreted. The more that is excreted, the better the liver is working.
This is a functional measure of the metabolic capacity of the liver. Exalenz has shown a correlation between liver damage and cirrhosis and the 13C-methacetin metabolic capacity. They’ve also shown that it is related to patient outcomes.
As these two tests are further refined and evaluated, they could become important in diagnosing and monitoring the treatment of liver disease, because they aren’t just looking at the structure of the liver, but they actually give us a sense of how liver function is changing.
Between serum, imaging and functional tests, there may soon be a wide range of reliable and non-invasive tests available to us. Each of these tests measures different things, so they’re likely to be used in combination. I can envision using an imaging test to look at the structure of the liver and a functional test to determine liver function. In our NASH-CX trial, that’s why we have the hepatic venous pressure gradient (HVPG), liver biopsy, FibroScan® and the 13C-methacetin breath test from Exalenz. I will discuss HVPG and why we are using this test in a future Perspective.
Our clinical trials are testing GR-MD-02, but at the same time we’re also evaluating the relevance of certain non-invasive tests. From my perspective, this is something that all companies developing treatments for NASH and liver fibrosis should incorporate into the design of their clinical trials. No matter what the results for the candidate drugs, we should also take the opportunity to gain a better understanding of how the results of non-invasive tests correlate to the results of a liver biopsy and disease progression. That would add tremendous momentum in this area of medicine and with improved diagnosis, it would support the commercial sales of these drugs when approved.
- HepQuant products are investigational combination drug and in vitro diagnostic devices and have not yet been evaluated or reviewed by the U.S. Food and Drug Administration (FDA). They are not currently available for clinical or investigational use or commercial sale.
- The Exalenz breath test is not currently approved in the U.S. for the assessment of liver function.
These “CEO Perspectives” are a regular feature of our communication activities and may contain forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “might,” “could,” “expect” and others. These statements include those regarding the hope that Galectin Therapeutics’ development program for GR-MD-02 will show that it can be both safe and effective in the treatment of liver disease, including NASH. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Make a Comment or Ask a Question
[contact-form-7]The post Developing Tests to Assess Liver Function in NASH and Cirrhosis appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Fatty liver disease: Motivation to lose weight appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>Are you one of the nearly 40% of Americans classified as obese or are you overweight and inexorably headed towards obesity? Has your physician ever suggested you lose weight or have you made a New Year’s resolution to go on a diet? Do you need any more motivation to lose weight? If you do, here’s one: losing weight can reverse fatty liver disease and keep your liver healthy. And the good news is you don’t have to lose all that much weight to see a major improvement.
In fatty liver disease – also known as non-alcoholic steatohepatitis, or NASH – fat globules accumulate in liver cells, leading to the death of some of those cells and the development of an inflammatory reaction. With years of chronic inflammation, scar tissue begins to form in the liver via a process called fibrosis. When the scar tissue becomes severe, a condition called cirrhosis, the liver architecture becomes distorted and the blood flow to the liver is altered, resulting in life-threatening complications and liver failure.
The prevalence of NASH has reached epidemic proportions with as many as 25 million U.S. adults having the disease, as reported in a recent Newsweek article entitled “NASH is the 21st century’s looming public health threat.” I was interviewed for this article, and Galectin Therapeutics and our NASH therapeutic GR-MD-02 have a prominent place in the discussion. The article accurately reflects the critical aspects of this disease. Specifically, in its early stages with mild fibrosis, the disease can be improved with lifestyle changes including weight loss. However, when fibrosis is advanced, and particularly when cirrhosis is present, weight loss has much less effect and the only resort may be a liver transplant. This is why our drug treatment is focused on patients with advanced fibrosis and cirrhosis.
Now let’s get back to the good news. If you have early stage NASH – meaning you have inflammation with early stages of fibrosis – weight loss will significantly improve the health of your liver. In a recent clinical study, all patients who lost at least 10% of their body weight had reductions in their fatty liver disease on liver biopsy, with 90% having complete resolution of NASH. Additionally, patients who lost less weight, including as little as 3% of their body weight, also had significant improvements. In all patients who lost weight, every aspect of NASH was improved including fat in liver cells, liver cell death, and inflammation. It is important to note 61% of the patients in this study had no fibrosis, and it was mild in those that had fibrosis.
As described in the Newsweek article, I can personally affirm that weight loss can improve one’s liver. An ankle injury I suffered during a college football practice resulted in multiple surgeries and forced me to stop exercising, and I gained a significant amount of weight – in the neighborhood of 50 pounds. This resulted in high blood sugar and elevated liver enzymes, indicating potential damage to my liver due to fatty liver disease. My physician prescribed anti-diabetic medication, but I decided it was best to focus exclusively on losing weight. I was successful in losing approximately 10% of my body weight, and I’m continuing to lose.
While I am not yet at my ideal body weight, the improvements are dramatic. My blood glucose is now normal and stays normal throughout the day (and I’m not taking diabetes medication), and my liver enzymes have decreased and are now within the normal range. Also, I feel much better and my clothes fit! The important point is that you do not need to get all the way to your ideal weight to see dramatic improvements in liver health and other important health benefits. This is not an all-or-nothing proposition, and every little bit helps.
If you are one of those people carrying around extra weight, get started losing weight now. It doesn’t take much weight loss to improve your liver health. There are many approaches to losing weight, which you should discuss with your healthcare provider. And don’t forget to combine your weight loss program with exercise, which has also been shown to improve liver health. I will return to a number of the important issues raised in the Newsweek article in future Perspectives. In the meantime, I’ll see you at the salad bar.
These “CEO Perspectives” are a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “might,” “could,” “expect” and others. These statements include those regarding the hope that Galectin Therapeutic’ s development program for GR-MD-02 will show that it can be both safe and effective when used in combination with other drugs for the treatment of patients with cancer. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements.
Footnotes:
- Defined as a BMI over 30; BMI = weight (in pounds) x 703 ÷ height (in inches) ÷ height (in inches)
- Available online as of January 30, 2015 and in the print edition dated February 12, 2016
Make a Comment or Ask a Question
[contact-form-7]The post Fatty liver disease: Motivation to lose weight appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Are You Eligible for the Galectin Therapeutics’ NASH Cirrhosis Trial? appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>In June 2015 Galectin Therapeutics initiated a clinical trial to determine if our investigational drug GR-MD-02 can successfully treat patients with severe scarring of the liver (cirrhosis) due to fatty liver disease (a.k.a. nonalcoholic steatohepatitis, or NASH). The goal of the study (the NASH-CX trial) is to assess whether GR-MD-02 may reduce the fibrous tissue that is clogging the liver in subjects with NASH cirrhosis. A reduction, in turn, is expected to improve liver function and have a positive effect on patient outcomes, such as perhaps delaying or avoiding a liver transplant. Please see my earlier CEO Perspective, “Clinical Trial to Establish Efficacy of GR-MD-02 in NASH Cirrhosis,” where this study is described in more detail.
Can you participate in this clinical trial?
If your cirrhosis is caused by NASH and you have portal hypertension, but you haven’t developed other complications related to your cirrhosis, then you might be eligible to participate in this trial. You must be between 18 and 75 years old and meet various other study eligibility requirements. This study is limited to people with cirrhosis only caused by NASH and not by any other factors, like alcohol or hepatitis.
If you qualify, you would be one of 156 participants at about 45 to 60 study sites, or clinics, across the United States. It is important to remember that this is an experimental study comparing GR-MD-02 against a placebo; the trial design is such that you have 2 out of 3 chances of being on active drug and 1 out of 3 chances of being treated with placebo.
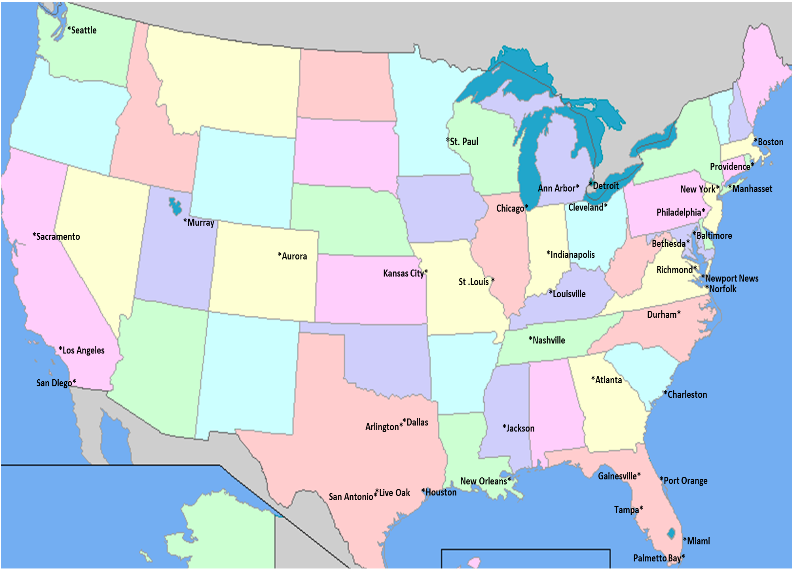
The study medication will be administered by an intravenous infusion every two weeks for one year. We expect that each clinic visit will last about an hour and a half. Below you will find a map showing the cities where the study is being conducted to see if you are able to make it to the site every two weeks. If you think you might be eligible for our study, please contact one of the study sites (click here for the list of sites and the appropriate contact information).
More information about this trial can be found at clinicaltrials.gov:
• NASH-CX: https://clinicaltrials.gov/ct2/show/NCT02462967?term=GR-MD-02&rank=3
Should the NASH-CX trial be successful, this will be the first clinical study of an investigational drug candidate to show a reduction of fibrosis in people with cirrhosis and the first hope of a future approved treatment other than a liver transplant.
These “CEO Perspectives” will be a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “could,” “expect” and others. These statements include those regarding the hope that Galectin’s development program for GR-MD-02 will lead to the first therapy for the treatment of fatty liver disease with advanced fibrosis and cirrhosis. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements
Please look for future editions in which multiple aspects of our development programs for unmet medical needs will be addressed.
GT-026 STUDY SITE MAP
Make a Comment or Ask a Question
[contact-form-7]The post Are You Eligible for the Galectin Therapeutics’ NASH Cirrhosis Trial? appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Why Fibrosis is a Hot Area for Pharmaceutical Research appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>Bristol-Myers Squibb ($BMS) recently paid $150 million for the exclusive right to acquire Promedior, a clinical-stage biotechnology company in the midst of a Phase 2 trial on the treatment of idiopathic pulmonary fibrosis (IPF) and myelofibrosis (MF). If clinical trials are successful, the deal could be worth as much as $1.25 billion. This is just one of a number of fibrosis-related acquisitions for BMS over the past few years, and BMS is not the only company active in this market. Fibrosis is a hot area right now. But why so?
The scientific community has known for a long time that fibrosis is a common final pathway for many different diseases. An investigator at the NIH suggested in 2004 that as many as 45 percent of the deaths in the United States are related to fibrosis (1). That would include, in addition to liver fibrosis, heart, kidney, lung, skin, and arterial fibrosis – all organs that can be scarred as the result of a chronic disease, which then leads to organ failure and death.
While we can certainly work on curing each individual chronic disease that causes fibrosis, another approach would be to inhibit the fibrotic process. This approach could potentially be applied to a lot of other diseases as well — it’s been something of a Holy Grail in medicine for decades.
It’s a great idea. Unfortunately, there hasn’t been very much progress in the development of anti-fibrotic agents, until now.
Recently, there has been promising work in agents that appear to inhibit fibrosis — for example, our own GR-MD-02, which in our preclinical studies has shown to not only prevent fibrotic damage, but even reverse it. I think these breakthroughs are happening now because the medical community is coming to understand that fibrotic diseases, such as NASH, are complex conditions that require agents that affect multiple pathways in the fibrogenic process.
Let me give an example. There are many important cytokines in the inflammatory process, so it might make sense to inhibit one of them and see how that changes the inflammatory or the fibrotic process. However, by doing that, you are ignoring dozens of other cytokines that are also involved in the inflammatory process. Even if you inhibit the one, you’re not having any impact on the other cytokines involved.
Therefore, agents that address a number of different cell types in the liver that express a wide range of cytokines and fibrotic mediators may be more effective than a pinpoint attack on a particular cytokine or mediator. GR-MD-02 appears to affect macrophages as well as activated myofibroblasts in the liver, which inhibits a wide range of different fibrotic processes. It may be that affecting master regulatory cells involved in inflammation and fibrosis is going to be more effective than affecting any individual mediators.
But as I pointed out, fibrosis is a problem in many other organs than the liver. My sense of it is, if you’re going to have a drug that is robust for a particular organ fibrosis, it’s more than likely going to work for other fibrotic diseases. That’s one of the reasons why we have done pre-clinical studies of GR-MD-02 in lung, kidney and heart, and it’s shown an effect in those as well. That is also, I suspect, part of BMS’ calculations in acquiring Promedior. IPF and lung fibrosis is an indication that creates a large enough market on its own, but the potential to address a disease process involved in 45 percent of the deaths in the U.S. can be found in the background of any fibrosis drug.
That is one of the things that makes GR-MD-02 different than many of the other drugs being developed to address NASH and fatty liver disease. Most of the dozen or so compounds don’t address the core fibrotic process, so even if they work in NASH, they’re not likely to work elsewhere in the body. Only the truly anti-fibrotic drugs like GR-MD-02 have the potential to address fibrosis in other organs.
These “CEO Perspectives” will be a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may”, “could”, “expect” and others. These statements include those regarding the hope that Galectin’s development program for GR-MD-02 will lead to the first therapy for the treatment of fatty liver disease with advanced fibrosis and cirrhosis. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements
Please look for future editions in which multiple aspects of our development programs for unmet medical needs will be addressed.
Reference List
- Wynn TA. Fibrotic disease and the T(H)1/T(H)2 paradigm. Nat Rev Immunol 2004 Aug;4(8):583-594.
Make a Comment or Ask a Question
[contact-form-7]The post Why Fibrosis is a Hot Area for Pharmaceutical Research appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Lessons Learned from the Failure of Raptors’ Phase 2b NASH Trial appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>On September 14, 2015, Raptor Pharmaceutical Corp. (NASDAQ: RPTP) announced top-line results of its Phase 2b trial evaluating RP103 in children with biopsy-confirmed nonalcoholic steatohepatitis (NASH). As reported here, the study failed to meet its primary endpoint of a two-point decrease in a fatty-liver-disease scoring system and no worsening of fibrosis, or scarring of the liver. It’s always disappointing when a promising drug candidate fails in a clinical trial, especially when it addresses something like NASH, for which there really aren’t any proven treatment options.
The failure of the Raptor trial provides an important lesson for any company developing therapies to address fatty liver disease and NASH on the use of surrogate blood markers in tracking the progression (or regression) of fatty liver disease and NASH.
If you’ve ever had routine blood work done as part of a physical, the tests probably included the measurement of the transaminases AST (aspartate aminotransferase) and ALT (alanine aminotransferase). These are enzymes that naturally circulate in the blood. They are also enzymes that are in cells and, in particular, they are in liver cells. If there is damage to the liver, as with a viral hepatitis A infection, these enzymes will be released into the blood serum in great numbers. A marked increase in the transaminases in your blood is one of the ways doctors diagnose hepatitis and other liver diseases.
Transaminases are often elevated in fatty liver disease and NASH. If you recruit a group of NASH patients, on average, the liver enzymes are going to be elevated. It’s easy to make the logical conclusion that if you have a drug that might work in NASH, and you treat those patients, the transaminase levels should come down. A number of trials have been undertaken with that presumption, and one of them was Raptor’s.
Between 2008 and 2010, Raptor conducted a small, open-label trial (meaning there wasn’t a placebo arm in the trial) with its drug – a long-acting, slow-release cysteamine – in adolescents with NASH (mean age 14). Eleven patients completed the trial and seven patients had either normalization or >50% reduction of their transaminase (ALT) level from baseline. These results led the investigators to suspect the drug was having activity in NASH. They quickly moved on to the latest Phase 2b study; Raptor even received the support of the National Institutes of Health (NIH), which agreed to conduct and help fund the trial.
In this newest study, the transaminase levels of the patients indeed went down, but liver biopsies showed no change in the histology of that organ. This is evidence that the changes in transaminase levels seen in NASH patients are not necessarily indicative of the activity of the underlying disease. While there may be a correlation with some treatments, this trial shows that this is not always the case. In reality, patients with fatty liver disease and NASH will see their levels of transaminases fluctuate widely. Roughly two-thirds of all patients, at any given time, will have normal transaminases. There’s no good evidence that transaminases correlate with either the stage or the activity of the disease.
This failure of the Raptor study also has a broad implication for all clinical trials involving NASH because it demonstrates that serum transaminases cannot be relied upon as an early biomarker of the effectiveness of a drug. It may also have ramifications for other potential biomarkers. The lesson from Raptor’s failure shows that we need to be skeptical about serum biomarkers until they’re well correlated with changes in the liver itself.
Here at Galectin we are ever mindful of the need to correlate biomarkers with disease and how difficult the task is. In our Phase 2 program in NASH with advanced fibrosis and cirrhosis, we are performing multiple tests to ensure we have correlation with the underlying disease. In the NASH-CX trial we are performing both invasive (including biopsy) and non-invasive physical and metabolic tests to evaluate correlation (see discussion here) and the NASH-FX trials utilizes three of the most promising methods for non-invasive imaging methods to assess physical properties of the liver that correlate with fibrosis (see discussion here).
While not every clinical trial ends with success, they all help advance our understanding of fatty liver disease and NASH. It’s just a matter of learning the lessons they teach us.
These “CEO Perspectives” will be a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “could,” “expect” and others. These statements include those regarding the hope that Galectin’s development program for GR-MD-02 will lead to an additional therapy for the treatment of psoriasis. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements
Please look for future editions in which multiple aspects of our development programs for unmet medical needs will be addressed.
Make a Comment or Ask a Question
[contact-form-7]The post Lessons Learned from the Failure of Raptors’ Phase 2b NASH Trial appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>The post Lead product candidate GR-MD-02 shows no unfavorable drug-drug interactions appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>An important question in drug development, and the subject of U.S. Food and Drug Administration (FDA) regulations, is whether a drug candidate interacts with other medications the target patient population may also be taking. This is a critical issue, because many patients with chronic diseases are on multiple medications over long periods of time and may take other medications on an intermittent basis.
The basis of many drug-drug interactions is that the experimental new drug may use some of the same metabolic pathways that other drugs use. If this is the case, the new drug may inadvertently increase the levels of other drugs in the system, and thus alter their effect and increase their side effects. Prescribing physicians need to know about potential unfavorable interactions, if any, between an experimental new drug like GR-MD-02 and other drugs their patients may require.
In evaluating potential drug interactions, the first experiments with GR-MD-02 were done in test tubes and with cell cultures. Many metabolic pathways were evaluated in this way to determine whether there were potential interactions with GR-MD-02. Generally, the results of these experiments showed there was little to no risk of drug metabolism interactions with GR-MD-02, but the analysis of one particular metabolic enzyme, called CYP3A4, suggested there was small risk for interaction with other drugs. Therefore, the company agreed with the FDA to evaluate the possible interaction in humans of GR-MD-02 with a model drug for the CYP3A4 enzyme. The model drug used was midazolam, which is known as Versed® and is widely used for mild, conscious sedation.
We designed, conducted, completed, disclosed publicly (see our press release dated May 14, 2015) and reported to the FDA results of a Phase 1 study in normal healthy volunteer subjects. This study first tested drug levels of midazolam after a single intravenous (IV) dose, which served as a control. Midazolam was then administered again and drug levels were monitored following a single IV dose of GR-MD-02 (8 mg/kg) and following three weekly IV doses of GR-MD-02 (also 8 mg/kg). A total of 17 subjects completed the study, and all met the primary endpoint of no difference between midazolam levels when administered alone and in combination with single and multiple doses of GR-MD-02. Of note, 8 mg/kg of body weight of GR-MD-02 is the same dose we are testing in our current Phase 2 program in nonalcoholic steatohepatitis (NASH) patients with cirrhosis and with advanced fibrosis.
These Phase 1 results show that GR-MD-02 has no effect on the metabolism and serum levels of midazolam, and these results can be imputed to other drugs metabolized by CYP3A4 that are in common use. In fact, the CYP3A4 enzyme metabolizes about half of all the drugs currently on the market, according to published estimates. (Click here for more information on CYP3A4.) With the successful completion of this study, the company does not anticipate further drug-drug interaction studies will be required.
So, what does this science mean for the development of GR-MD-02? First, another 17 healthy individuals received up to three doses of GR-MD-02 without any significant adverse events, confirming the safety of the drug as seen in the first Phase 1 trial. Second, these findings allow patients on concomitant medications to be enrolled in our Phase 2 clinical trials with minimal concern for drug interactions, thus increasing the pool of potential patients that can be included in the trials. Finally, should GR-MD-02 receive marketing approval, patients and physicians will be less concerned our drug will interfere with other drugs they may be taking and we will not be faced with restrictive labeling regarding concomitant drug therapy. Therefore, successful completion of this drug interaction study in people checks another box in describing the underlying properties to support approval of GR-MD-02.
These “CEO Perspectives” will be a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “could,” “expect” and others. These statements include those regarding the hope that Galectin’s development program for GR-MD-02 will lead to the first therapy for the treatment of fatty liver disease with advanced fibrosis and cirrhosis. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements
Please look for future editions in which multiple aspects of our development programs for unmet medical needs will be addressed.
Make a Comment or Ask a Question
[contact-form-7]
The post Lead product candidate GR-MD-02 shows no unfavorable drug-drug interactions appeared first on NASH & Liver Fibrosis | Galectin Therapeutics.
]]>