

Written by Peter G. Traber, M.D. on September 2, 2015
In late June 2015, Galectin Therapeutics initiated a Phase 2 clinical trial (the NASH-CX trial) to evaluate the ability of its anti-galectin drug GR-MD-02 to treat patients with cirrhosis of the liver due to fatty liver disease (non-alcoholic steatohepatitis, or NASH). Cirrhosis is advanced-stage scarring, or fibrosis, in which the liver is “clogged” with fibrous tissue that distorts the organ’s architecture and results in increased resistance to blood flow to the liver and dysfunction of liver cells. The goal of therapy with GR-MD-02 is to reduce fibrosis and, in turn, improve liver function and positively affect patient outcomes.
One of the most important aspects of any clinical trial is the “endpoint” that will be measured as evidence of the drug’s effect. Endpoints include the “primary” endpoint on which the overall success of the trial is based, and “secondary” endpoints that are supportive of the primary endpoint. The strongest endpoints for any clinical trial are those related to patient outcomes which include how a patient feels, functions, or survives (mortality). However, these endpoints in chronic diseases often can only be measured in the end stage of disease, which often occurs many years after the patient contracts the disease. Therefore, many clinical trials are conducted with surrogate endpoints that are linked to patient outcomes. For drugs such as GR-MD-02 that fulfill a significant unmet need, the U.S. Food and Drug administration (FDA) may allow the initial approval of drugs based on achieving a reasonable surrogate endpoint under an accelerated approval pathway.
For NASH cirrhosis, potential surrogate endpoints have been proposed by experts in the field in joint discussions with the FDA (1) including measurement of change in hepatic venous pressure gradient (HVPG), which is a measure of pressure in the main blood supply to the liver (viz., portal pressure). In the NASH-CX trial, we are using a reduction in HVPG as the primary endpoint for evaluating efficacy. Secondary endpoints in the study, some of which are also potential surrogate endpoints that have been discussed with the FDA, include liver biopsy evaluations of fibrosis, non-invasive diagnostic tests including FibroScan® to measure liver stiffness, which correlates with fibrosis, and the 13C-methacetin breath test (MBT, Exalenz Bioscience Ltd.) (2), which is a measure of liver metabolic function. Further secondary endpoints also include direct patient outcome measures related to complications of cirrhosis. We believe, based on our discussions with the FDA, that these endpoints will provide a broad and relevant set of measures to determine whether GR-MD-02 could be an effective therapy for NASH cirrhosis.
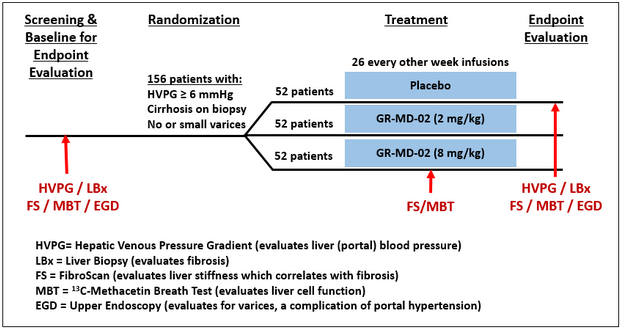
While a clinical trial protocol such as the NASH-CX trial is a detailed and complicated document (nearly 250 pages long in our case), the fundamentals are straightforward, as shown in the figure below. All patients enrolled do have cirrhosis and portal hypertension, but are well-compensated, meaning that they have not yet had complications related to their cirrhosis. Patients who meet the inclusion and exclusion criteria will be randomly allocated to receive either placebo or one of two doses of GR-MD-02. The trial is double-blinded, meaning neither the patients nor their physicians, nurses or Galectin Therapeutics will know what therapy they are receiving. The various diagnostic evaluations will be done as indicated in the figure and for each patient the changes in these evaluations at the end of treatment will be compared with the evaluations performed at the beginning of the study. The length of the study is related to the duration of GR-MD-02 treatment as well as the number of patients in the study to achieve a necessary sample size for scientific and statistical evaluations. For this study, a total of 156 patients will each receive either a dose of GR-MD-02 drug or placebo in biweekly infusions for one year.
A number of investors have asked about the actual conduct of the clinical trial, so I will provide some details. We have engaged a large, multinational contract research organization (CRO) that is experienced in performing studies in liver disease, NASH, and cirrhosis. All study sites will be in the U.S. and will include a mix of large academic centers with internationally recognized clinical experts and prominent community-based health care centers. The two co-principal investigators for the trial, Dr. Naga Chalasani from Indiana University and Dr. Stephen Harrison from San Antonio Military Medical Center, are recognized experts in the field and were investigators in our Phase 1 clinical trial in NASH patients with advanced fibrosis.
Our most important operational milestone is the last patient randomized, in other words the first infusion of drug or placebo for patient number 156, which is targeted for August 2016. With a one-year treatment phase, if we meet this milestone then all patients will have completed therapy as of August 2017, with a goal for reporting top-line data by the end of 2017. Using the experience of our CRO in other trials of this type, we believe that we may achieve this goal with 45 study sites, but are able to increase that number to 60 study sites if necessary to stay on schedule. At this time, we have identified and pre-certified 55 study sites across the U.S., and are rapidly engaging to a total of 45 fully active study sites.
Fully establishing sites to enroll patients includes gaining approval from each of their investigational review boards (IRB), clinical and indemnification contracts, financial contracts, and education and training of their personnel. After sites are initiated, patients are screened in a process that involves performing multiple laboratory tests at different times, various invasive tests such as an upper endoscopy (EGD), liver biopsy and HVPG, and non-invasive tests such as FibroScan and MBT; this testing alone may take up to eight weeks. Assuming a patient passes the various screening parameters for entry into the trial from all these tests, they are then randomized and begin receiving bi-weekly infusions of drug or placebo. Sites are currently screening, enrolling and treating patients.
What do we expect to learn from this study? First, we expect to learn whether GR-MD-02 can reduce the portal pressure in a patient population of well-compensated cirrhosis, a measure that is known to be directly related to complications of cirrhosis and patient mortality. Second, we expect to learn whether our drug reduces portal pressure by reducing the amount of scarring in the liver as determined by liver biopsy. Finally, we anticipate learning how a reduction in fibrosis and portal pressure correlates with non-invasive testing such as FibroScan, MBT, serum biomarkers and other tests including a quality-of-life questionnaire and complications of cirrhosis. The NASH-CX trial is a rigorously designed study to gain the most information possible regarding the effect of GR-MD-02 in these patients, who have no current available therapy. The NASH-CX trial also importantly serves to help design later-stage trials such as those that may be required for regulatory approval. With success in this trial, GR-MD-02 could be the first drug shown to reduce fibrosis in cirrhotic patients and the first hope of a treatment in this patient population other than liver transplant.
More information on Galectin’s NASH-CX trial can be found at clinicaltrials.gov
- NASH-CX: A Multicenter, Randomized, Placebo-controlled, Double-blind, Parallel-group, Phase 2 Clinical Trial to Evaluate the Safety and Efficacy of GR-MD-02 for the Treatment of Liver Fibrosis and Resultant Portal Hypertension in Patients With Nash Cirrhosis https://clinicaltrials.gov/ct2/show/NCT02462967?term=GR-MD-02&rank=3
These “CEO Perspectives” will be a regular feature of our communication activities and may contain forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements relate to future events and use words such as “may,” “could,” “expect” and others. These statements include those regarding the timing of enrollment of patients and the hope that Galectin’s development program for GR-MD-02 will lead to the first therapy for the treatment of fatty liver disease with advanced fibrosis and cirrhosis. For a discussion of additional factors impacting Galectin’s business, see the Company’s Annual Report on Form 10-K for the year ended December 31, 2014, and subsequent filings with the SEC. You should not place undue reliance on forward-looking statements. Although subsequent events may cause its views to change, management disclaims any obligation to update forward-looking statements
Reference List
1. Sanyal AJ, Friedman SL, McCullough AJ, Dimick-Santos L. Challenges and opportunities in drug and biomarker development for nonalcoholic steatohepatitis: findings and recommendations from an American Association for the Study of Liver Diseases-U.S. Food and Drug Administration Joint Workshop. Hepatology 2015 Apr;61(4):1392-1405.
2. Exalenz Bioscience Ltd. (Israel). See www.exalenz.com for information on Exalenz and the 13C-methacetin breath test



